By Brian Kitzerow, PT, DPT, OCS, CMPT
Pain in hypermobility is real, explainable, and treatable. Highly flexible people can sometimes have a large amount of pain but have a very difficult time finding care and support to treat their discomfort. Their doctors might not be able to identify any causes for the pain and this can lead to feelings of alienation and inadequacy. This isn’t necessarily because there isn’t anything wrong with them, but more commonly it is because medical clinics don’t have the same tools our research labs have to identify dysfunctions that cause the pain. X-rays and MRIs are excellent for major structural injuries, but they cannot detect dysfunction at the level of nociceptors, small fibers, proprioceptors, or subtle instability.
Likewise, pain in hypermobility isn’t simple — and it isn’t easily communicated. Like the experience of seeing color, pain is highly individualized. Two people can look at the same object and agree that it’s red, yet their internal experience of ‘redness’ is shaped by their biology, past experiences, and neural wiring.
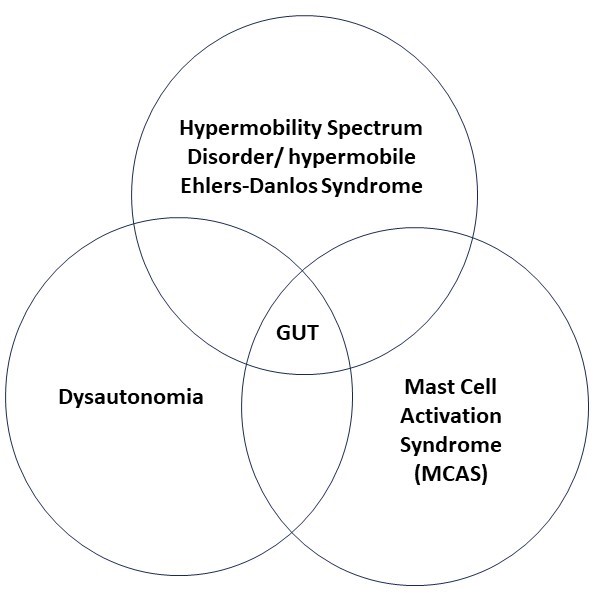
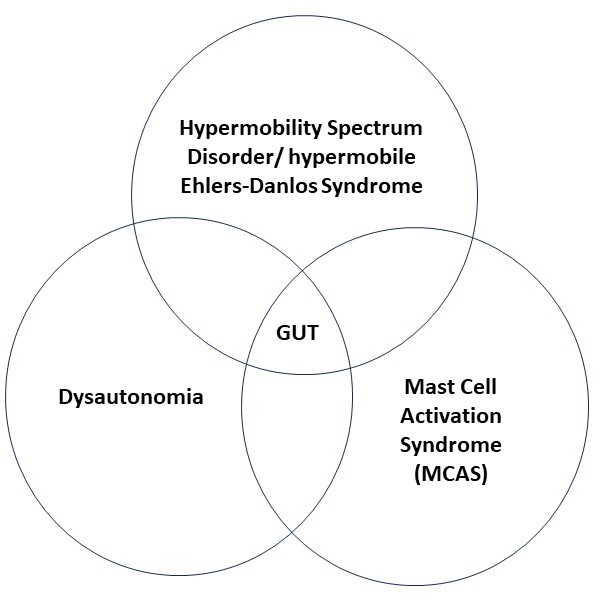
Additionally, pain in hypermobility arises from many different pathways, not just “loose joints.” Contributing factors may include:
- Immune reactivity or autoimmune overlap
- Increased muscle, tendon, and ligament strain
- Central sensitization
- Dysautonomia / POTS
- Small fiber neuropathy
- Peripheral nerve strain
- Brainstem and spinal cord stress
- Sleep disruption
- Hormonal cycling
- Dietary triggers
- Psychological stress
That’s a big list and it can be very difficult to negotiate that experience on your own.
Hypermobility vs Hypermobile Spectrum Disorders
Hypermobility alone is not a disorder. Hypermobile joints are a normal variation of the human population. Like Yin and Yang you cannot define a person as stiff without having the contrast of loose. The evolution of individuals with “looser” musculoskeletal systems brings with it certain hypothetical advantages that have maintained the genetic expression in our population. But with these advantages come risks.
Likewise, unlike disorders caused by single-gene mutations, hypermobility appears to arise from complex interactions among multiple genes. A characteristic of genetic diseases is that a defect in a single or small number of genes can cause the function of the body to fall off the rails. In Marfan’s it is FBN-1.[i] In Vascular EDS it is COL3A1.[ii] Classical EDS is associated with COL5A1 or COL5A2.[iii] Hypermobility, in contrast, is suspected to arise from interactions among multiple genes, although the exact genes remain unidentified. This suggests an evolutionary trend towards specific physical attributes rather than an accidental mutation.
We still do not have a strong consensus on how prevalent hypermobility is in the population. Opinions vary wildly with Blajwajs reporting that the number lies between 2 and 57% of the population being hypermobile.[iv] That’s a massive range with a great deal of uncertainty.
Some studies have looked at hypermobility in segments of our population[v][vi], but clarity on the entire population remains undefined. A synthesis of publications in the last 10 years on adults with a Beighton scale of >4/9 suggests a consensus of 16-22% of the population.[vii] An estimated one fifth of the population does not suggest an accidental genetic disease.
Hypermobility becomes a dysfunction rather than a normal presentation of a population when symptoms appear. Pain, dislocation, challenges with stability, fatigue, headache, etc. Again, the causes of symptoms developing are not homogenous across hypermobile populations and can arise from a multitude of causes and interactions.
Pain presentation models like Scott Dye’s Envelope of Function[viii] or Michael Turvey’s Tensegrity hypothesis[ix] are both deep dives, but highly powerful models for understanding when and why hypermobility raises the risks for transitioning from the healthy athlete to developing debilitating symptoms.
A Slice of Pain Generators
Ok, you’ve suffered through all the heavy theory. It’s time to get into relevant advice. Let’s look at four common causes of pain in hypermobility and what you can do about it. Keep in mind that most of these are models and are subject to change as our understanding evolves.
Micro-instability
Hypermobile joints have challenges “locking-in” to stable end-ranges. To compensate for this, the muscles in hypermobile individuals work harder to maintain neutral postures for sitting and standing. You might have noticed that it is easier for you to maintain standing positions by shifting around rather than standing at attention stiffly like other people can. This places more strain on the muscle and tendon structures and is more energy intensive.
Muscle strength is essential to compensate for this lack of stability. Deconditioning brings pain. Bracing can also be helpful.
Proprioception
We don’t know exactly why, but people with hypermobility have more challenges with proprioception. The decrease in end-range joint stability is almost certainly a contributor, but there are likely other causes that are being investigated as well.
We do know that when the brain has challenges identifying joint position it responds by increasing the protective tone that muscles rest at. This leads to stiffness, spasms and trigger points, even when you are at rest.
Helping your brain to know where your joints are can reduce these experiences. Weighted blankets, braces, tape, compressive clothing can all reduce energy expenditures and improve comfort. Somewhat counter-intuitively, exercise is extremely helpful to reduce this muscle stiffness. The more fit your muscles are the better they can maintain both joint stability and neurosensory tone.
Tendon and Ligament strain
Building on the first two factors, tendons and ligaments can experience more strain in a hypermobile system. The decreased end range stability and proprioception results in larger amplitude sway and delayed stabilization responses that increase strain on the tissues anchoring muscles and joints. This repeated low-grade strain often does not show up on imaging but still produces real pain.
Training and measures to protect those tissues can reduce the localized inflammation and pain. Again, bracing and taping is helpful. Increased muscular tone is also important. Finally, proprioceptive balance training can improve your ability to protect these tissues.
Central Sensitization
Pain is an adaptive experience that changes as we are exposed to different experiences, environments, stressors and stimuli. Research shows that we develop stronger neural pathways in the brain to experience pain when we regularly stimulate a particular pain pathway. This results in a lowered threshold for the nervous system to generate a pain response in association with that tissue. Occasionally these thresholds become low enough that a stress that causes no damage on the tissue level is experienced as excruciating pain.
Sometimes this is likened to the phenomenon of listening to music at higher or lower levels. After a short time, your brain adapts to the volume and you experience it in a normalized, mid-range. Pain pathways however are much more resilient and slower to adapt.
This does not mean that your pain is not real. It is very observable with brain imaging when a person is in pain. But it does mean that your nervous system is very skilled at creating a pain experience and that it would be more functional if the degree of stimulus to create a pain experience was more aligned with the degree of stimulus to cause tissue damage. Correct calibration would not only be less painful, but would help you to make better choices on what activities are risking tissue failure and which are not to prevent injury.
Central sensitization can be challenging to correct but we have solid research from clinicians like David Butler and Lorimer Mosely on pathways to correct it in the clinic.[x]
These are only a small sample of the different and highly complex mechanisms responsible for pain experiences in hypermobility.
With the right strategies, hypermobile bodies become stronger, more stable, and far less painful.
Evidence-based physiotherapy, pain education, strength training, and nervous-system regulation can dramatically improve comfort, function, and confidence.
If you’re living with hypermobility and pain, you’re not alone—and there is a clear, science-backed path forward.
[i] Dietz HC. Marfan Syndrome. In: Adam MP, Mirzaa GM, Pagon RA, et al., eds. GeneReviews® [Internet]. Seattle, WA: University of Washington, Seattle; 1993–2024. Updated 2017.
[ii] Murray ML, Pepin M, Byers PH. Vascular Ehlers-Danlos Syndrome. In: Adam MP, Mirzaa GM, Pagon RA, et al., eds. GeneReviews® [Internet]. Seattle, WA: University of Washington, Seattle; 1993–2024. Updated 2014.
[iii] Malfait F, Wenstrup RJ, De Paepe A. Classic Ehlers-Danlos Syndrome. In: Adam MP, Mirzaa GM, Pagon RA, et al., eds. GeneReviews® [Internet]. Seattle, WA: University of Washington, Seattle; 1993–2024. Updated 2017.
[iv] Blajwajs L, Williams J, Timmons W, Sproule J. Hypermobility prevalence, measurements, and outcomes in childhood, adolescence, and emerging adulthood: a systematic review. Rheumatol Int. 2023 Aug;43(8):1423-1444. doi: 10.1007/s00296-023-05338-x. Epub 2023 May 6. PMID: 37149553; PMCID: PMC10261186.
[v] Russek LE, Errico DM. Prevalence, injury rate, and symptom frequency in generalized joint laxity and joint hypermobility syndrome in a “healthy” college population. Clin Rheumatol. 2016;35(4):1029-1039.
[vi] Reuter PR, Fichthorn KR. Prevalence of generalized joint hypermobility, musculoskeletal injuries, and chronic musculoskeletal pain among American university students. PeerJ. 2019;7:e7625.
[vii] OpenAI. ChatGPT: Analysis of recent studies on generalized joint hypermobility prevalence in adult populations. December 2025. Accessed [date]. Available from: https://chat.openai.com
[viii] Dye SF. The knee as a biologic transmission with an envelope of function. Clin Orthop Relat Res. 1996;(325):10-18.
[ix] Turvey MT, Fonseca ST. The medium of haptic perception: A tensegrity hypothesis. J Mot Behav. 2014;46(3):143-187
[x] Moseley GL, Butler DS. Fifteen Years of Explaining Pain: The Past, Present, and Future. J Pain. 2015;16(9):807–813
About the author
Brian Kitzerow, PT, DPT, OCS, CMPT, is a new physiotherapist in Calgary with specialized expertise in hypermobility, Ehlers-Danlos Syndrome (EDS), dysautonomia/POTS, and complex pain conditions. With more than 15 years of clinical experience and advanced orthopedic credentials, Brian integrates biomechanics, pain science, and nervous-system regulation to help patients build stability, strength, and long-term resilience. He is dedicated to providing clear education, evidence-based treatment, and supportive care for individuals who often feel misunderstood in traditional medical settings.